Is Dry Needling Acupuncture?
Come at me, bro.
I am in a somewhat strange position in the acupuncture world.
There are many acupuncturists who specialize in treating orthopedic problems and musculoskeletal pain, and there are many acupuncturists who describe what they are doing as including dry needling. There are even a growing number of acupuncturists who have learned dry needling from PTs. But I am one of probably only a small handful of acupuncturists who also regularly teaches dry needling not only to acupuncturists, but also to physical therapists.
This means that I am regularly getting the opportunity to have productive, positive discussions with both acupuncturists and physical therapists (sometimes in the same room!) about what these words mean and how we are using them with our patients, and how to talk about this in a way that helps people. What I am finding is that the more of these discussions I participate in, the less sure I am about the best way to do it.
Add to that the growing animosity over the last ten or so years between acupuncturists and physical therapists about this topic, and the confusion in the general public about the differences between these types of therapy, and you create an environment where the stakes feel increasingly higher and higher, and the signal to noise ratio feels increasingly lower and lower.
Why definitions matter
In response to this situation, I decided to try to come up with a clean, rational way to define these terms. The difficulty really comes down to one basic question: why are we defining the terms in the first place? This might seem like a redundant question, but there are actually a few different possible reasons, including:
1) To sharpen professional boundaries and identities to try to attract more patients
2) To sharpen professional boundaries and identities to stay in our own lanes
3) To help the public find the right kind of treatment
4) To try to influence or limit what other professions are doing
But I am going to try to do something else: simply try to describe these practices as clearly and precisely as possible.
The first difficulty: what do we mean by the term “acupuncture?”
Does the term “acupuncture” refer solely to the modality of using acupuncture needles, or does it refer to an entire system of medicine based on East Asian theories of anatomy, physiology, and cosmology?
The most internally consistent approach that I have found is to limit the definition of acupuncture to the modality of using a filiform needle, i.e. an acupuncture needle, i.e. a sharpened length of steel wire, regardless of where you are putting it or why you are putting it there.
There are a few reasons for this. In terms of the rationale that many acupuncturists use for how they define acupuncture in this public debate, the most important one is that if we define acupuncture as a system of medicine based on traditional theories:
- An acupuncturist practicing modern acupuncture and not using traditional theories is by definition not practicing acupuncture (and therefore practicing outside of their scope of practice)
- A physical therapist practicing dry needling is by definition not practicing acupuncture
The second difficulty: public perception
The problem with this purely modality-based definition occurs when we bring in the public.
In the public’s mind (including within Asian communities), acupuncture is, most of the time, not separate from Chinese or other East Asian medical theory. In other words, if someone from the general public, with no prior experience of acupuncture goes to see an acupuncturist, they will usually expect that the acupuncturist will be assessing and treating them according to some kind of traditional theory.
This is why I’m limiting my discussion to trying to be as clear and precise with terminology as possible, for the purpose of having good quality discussions when we talk to each other as professionals. I am not suggesting that anyone, acupuncturist or physical therapist, starts using these definitions when talking to patients or the public.
One way around this problem is by separating the term acupuncture from the term acupuncturist. If we define acupuncture as a modality that involves the use of a particular tool and acupuncturist as someone whose professional license is primarily about their legal right to practice acupuncture, then that is good enough for this discussion.
And because it also happens to be the case that just about anyone who has a license to specifically practice acupuncture in this country has most likely also studied at least one form of traditional East Asian medical theory, in addition to maybe several forms of modern acupuncture such as dry needling or neurofunctional electroacupuncture, there is less danger of the public being confused about what an acupuncturist is.
But of course there is still the potential confusion around acupuncture vs acupuncturist in the public’s view; why would someone who is technically practicing acupuncture by this definition (e.g. a physical therapist doing dry needling) not automatically be called an acupuncturist?
So:
This is not a proposal for how we communicate with patients.
It is an attempt to clarify how we talk to each other as professionals.
Definitions: a work in progress
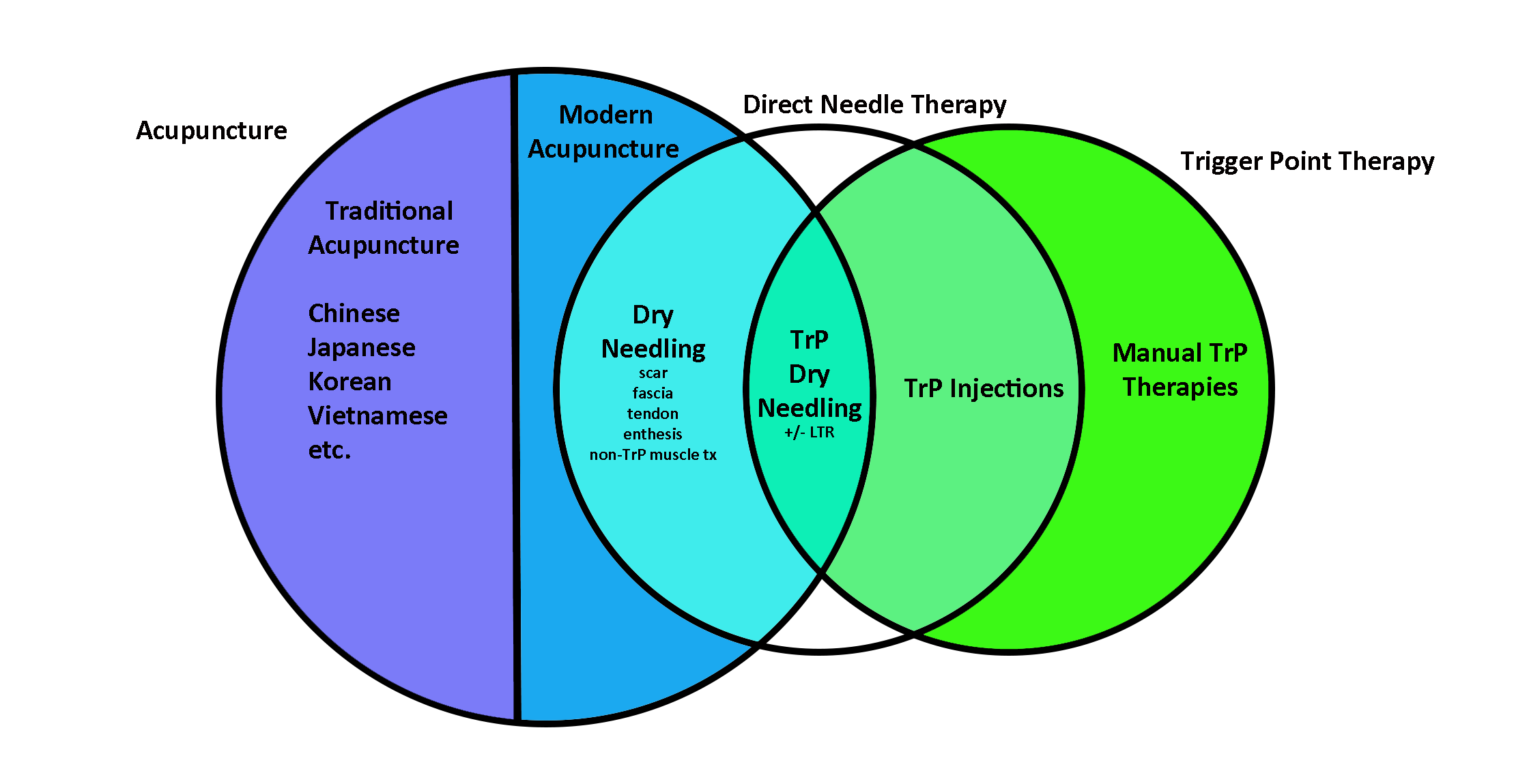
For this discussion, I’ve found it useful to think in terms of three overlapping categories:
- Acupuncture: the use of a filiform needle to create a therapeutic effect, regardless of where the needle goes or why you put it there
- Direct Needle Therapy: using any kind of needle (including hypodermic needles) to directly stimulate a bodily tissue that is pathological
- Trigger Point Therapy: any therapy focused on treating pain and dysfunction that is coming from trigger points, usually in muscle tissue
Within this way of looking at things, there are several subcategories within each of these three main categories, and this is where the overlapping happens.
Acupuncture can be roughly divided into two subcategories: traditional and modern.
- Traditional acupuncture: using traditional East Asian theories to decide where to insert needles and what to do to the needles once they are in place
- Modern acupuncture: using modern theories of anatomy and physiology to decide where to insert needles, including using modern theories to justify using traditional acupuncture points and channels
Of course, these subcategories are clear in theory, but in clinical practice, most acupuncturists blend them without even thinking about it. But I’m focusing here on pure terminology, not the rough, grey grittiness of clinical reality.
Example: an acupuncturist who puts needles in SI 11 and another one in the motor point of the flexor carpi ulnaris in order to treat a rotator cuff problem would be practicing a blend of traditional and modern acupuncture according to this definition.
Trigger Point Therapy includes any therapy aimed at treating trigger points, which can be various kinds of needling techniques like dry needling or trigger point injection, but also other forms of manual techniques like massage techniques, cupping, or spray-and-stretch.
In this schema, any kind of direct needle therapy that uses a filiform/acupuncture needle is by definition a form of modern acupuncture; this would include any kind of dry needling, whether it is targeting muscle tissue or some other tissue where the needle is being used primarily for its local effect on that tissue.
One weakness of the chart is that there should be an overlap between direct needle therapy and traditional acupuncture as well, which would create the category of “ashi” points, which are commonly used in traditional acupuncture. I couldn’t figure out a clean way of depicting that without making the chart messy, so I’ll leave that for a later revision of the chart. But for my current purposes, it doesn’t make too much of a difference.
Of course, there are going to be objections to any one way of defining these terms, so I thought I would acknowledge the main problems I can see with this particular diagram:
From the acupuncturist perspective: many acupuncturists have been very vocal about not using the term “dry needling” to denote a technique that is separate from traditional acupuncture, usually with the logic that goes something like:
“We are already doing dry needling; it’s what we learned in school, and the term dry needling was made up by physical therapists who want to appropriate our medicine and get away with it by calling it something else.”
I don’t find this line of reasoning convincing, for reasons I can go into in another blog entry, but I thought I would add it here because it is the most common reaction I’ve seen in response to other professions practicing dry needling.
From the physical therapist perspective: most physical therapists who I have learned from, trained alongside with, and taught, are very careful to say that what they are practicing is not acupuncture, and at Myopain Seminars, we tell physical therapists to not call what they are doing acupuncture. Although I think that at this stage this is the right thing to do in terms of public perception and professional boundaries, it is not a defensible position to take when we define acupuncture and acupuncturist in the way that I am suggesting.
Having said that, it would make total sense to make a distinction between an acupuncturist and a physical therapist, and that distinction preserves very reliable and meaningful differences in what the public could expect in terms of treatments if they went to see one kind of practitioner or the other.
Where to go from here
We keep talking, hopefully with the attitude of assuming the best motivations in each other, such as that what all of us are interested in is ultimately helping other people and pursuing the personal goal of clinical mastery. Does everyone have pure motivations? Of course not. But assuming that they do to start with seems like the only way to actually create a positive discussion. Clear definitions won’t eliminate disagreement, but they can at least ensure we are disagreeing about the same thing.